|
1
|
- Scott S. Emerson, M.D., Ph.D.
- Professor of Biostatistics,
- University of Washington
|
|
2
|
- Topics:
- Overview
- Frequentist approach
- Inferential methods
- Fixed Sample Clinical Trial Design
- Group Sequential Sampling Plans
- Evaluation of clinical trial designs
- Bayesian approach
- Inferential methods
- Probability models
- Nonparametric Bayes
- Evaluation of clinical trial designs
|
|
3
|
|
|
4
|
|
|
5
|
|
|
6
|
|
|
7
|
- Statistics is about science.
- Science is about proving things to people.
- Other scientists
- Community at large
|
|
8
|
- A well designed study
- Discriminates between the most important, viable hypotheses
- Is equally informative for all possible outcomes
- Binary search using prior probability of being true
- Also consider simplicity of experiments, time, cost
|
|
9
|
- Experimentation in human volunteers
- Investigate a new treatment / preventive agent
- Safety
- Efficacy
- Phase II (preliminary); Phase III
- Effectiveness
- Phase III (therapy); Phase IV (prevention)
|
|
10
|
|
|
11
|
- Collaboration among investigators to
- Define intervention
- Define patient population
- Define general goal
- Clinical measurement for outcome
- Relevant benefit to establish: Two or more of
- Superiority, noninferiority, approximate equivalence, nonsuperiority,
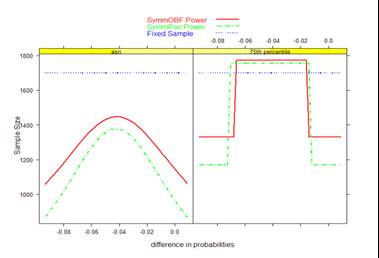
inferiority
|
|
12
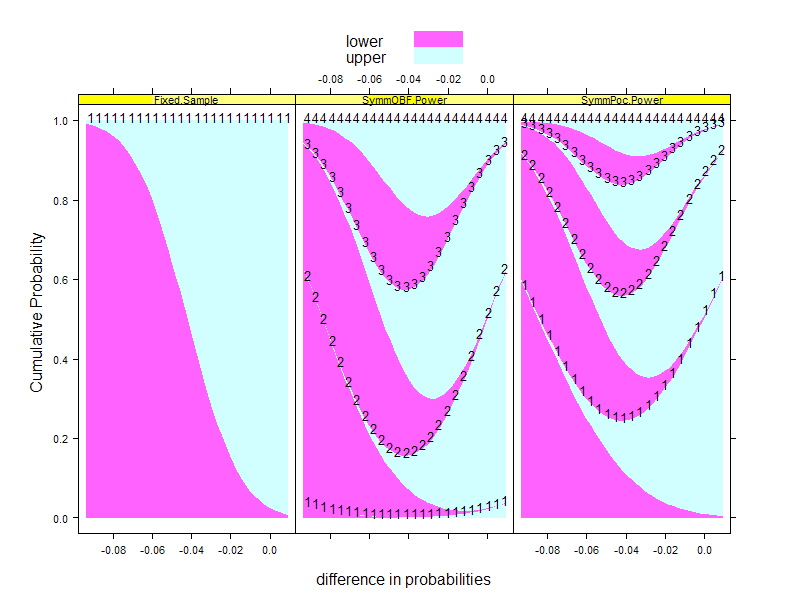
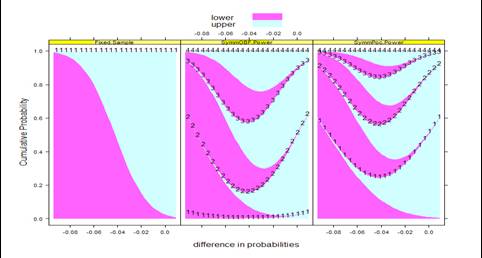
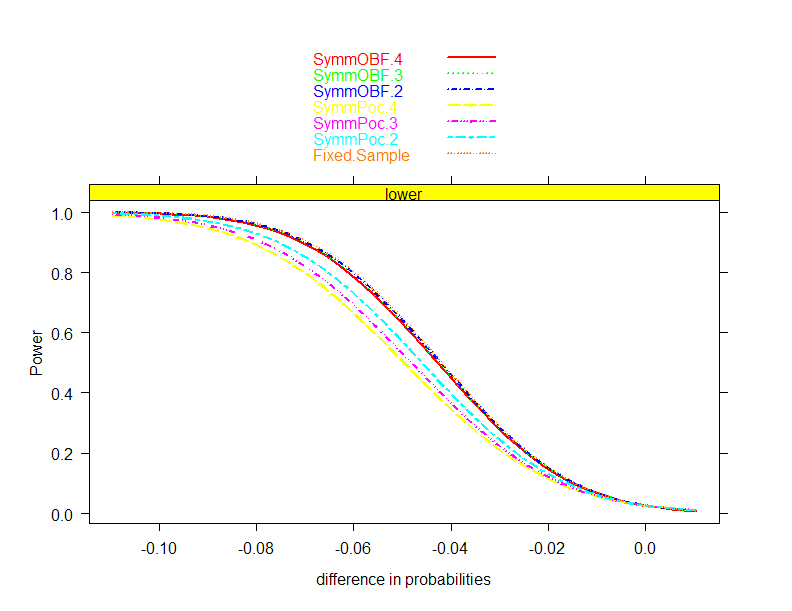
|
- The intervention when administered to the target population will tend to
result in outcome measurements that are
|
|
13
|
- Plan collection of a sample which allows
- Administration of intervention (ethically)
- Measurement of outcomes
- Statistical analysis of results
- Variability of subjects means that results need to be reported in
probabilistic terms
- Point estimate of summary measure of response
- Interval estimate to quantify precision
- Quantification of error rates for decisions
- (Binary decision?)
|
|
14
|
- In order to be able to perform analysis
- Modify intervention, endpoints to increase precision (without changing
relevance)
- Probability model for response
- Choose summary measure of response distribution
- Precise statement of hypotheses to be discriminated
- Stated in terms of summary measure
|
|
15
|
- Typical approaches to compare response across two treatment arms
- Difference / ratio of means (arithmetic, geometric, …)
- Difference / ratio of medians (or other quantiles)
- Median difference of paired observations
- Difference / ratio of proportion exceeding some threshold
- Ratio of odds of exceeding some threshold
- Ratio of instantaneous risk of some event
- Probability that a randomly chosen measurement from one population
might exceed that from the other
- …
|
|
16
|
- Issues when choosing statistical models
- Criteria for quantifying credibility of results
- Computational methods and formulas
- Covariate adjustment
- …
|
|
17
|
- Choice of statistical model impacts the scientific question actually
addressed as well as the statistical precision
- Robustness of inference depends on methods of computing the summary
measures to be compared
- Interpretation of positive and negative studies depends on computation
of sampling variance
|
|
18
|
- Where I Am Going:
- “A revolution no one will notice”
|
|
19
|
- Design and analysis of clinical trials to allow quantification of the
strength of evidence for or against scientific hypotheses
- AND to allow concise presentation of results
- Need to convince the audience, who may
- Disagree on what are most important hypotheses
- What precision is necessary for what endpoints?
- Disagree on definition of statistical evidence
- Frequentist vs Bayesian (with varying priors)
|
|
20
|
- I believe statistical methods should always take the scientific setting
into account
- Science ideally progresses through a series of experiments successively
addressing more refined questions
- I am against unnecessarily assuming the answer to more detailed
questions than I am trying to address in the scientific study
|
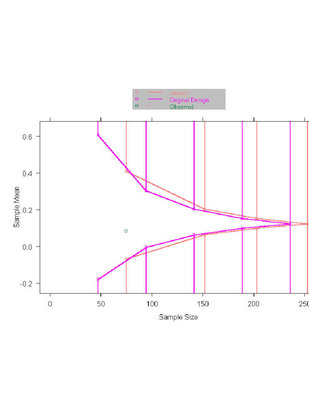
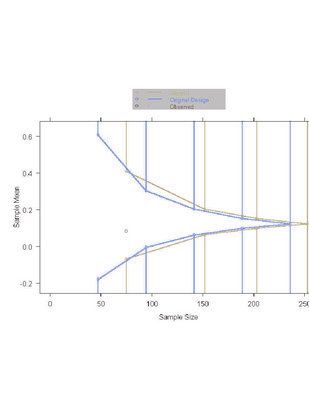
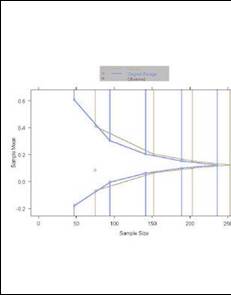
|
21
|
- There are two types of people in the world:
- Those who dichotomize everything, and
- Those who don’t.
|
|
22
|
- Breiman (2000): The two approaches to data analysis
- Model based vs algorithmic
- (e.g., regression vs trees, neural nets)
- This talk:
- Frequentist vs Bayesian
- (Semi)Parametric vs nonparametric
|
|
23
|
- Frequentist Methods
- Frequentist inference in fixed sample designs
- Probability models
- (Semi)parametric vs nonparametric
- Sequential sampling
- Bayesian Methods
- Bayesian paradigm
- “Coarsened” nonparametric Bayes
- Concise presentation of results
|
|
24
|
- Frequentist Inference
- in
- Fixed Sample Designs
|
|
25
|
- Hypothetical clinical trial
- Two groups: Treatment and Placebo
- Primary outcome variable: continuous
- Notation
|
|
26
|
- We choose some summary measure of the difference between the
distributions of response across the treatment arms
- Criteria (in order of importance)
- Scientifically (clinically) relevant
- Also reflects current state of knowledge
- Intervention is likely to affect
- Could be based on ability to detect variety of changes
- Statistical precision
|
|
27
|
- A common choice: Difference in means
- Why?
- Occasionally most relevant (health care costs)
- Sensitive to a wide variety of changes in distribution of response
- Statistically most efficient in the presence of normally distributed
data
|
|
28
|
- Design experiment by looking to the future: Consider how the results of
the study will be reported
- The single “best” estimate of treatment effect
- An interval estimate to quantify precision
- A quantification of the strength of evidence for or against particular
hypotheses
- Our conclusion from the study
|
|
29
|
- Define hypotheses to be discriminated
- Decisions for superiority or not sufficiently superior
- (One-sided test can also be defined for one-sided lesser alternative)
|
|
30
|
- Define hypotheses to be discriminated
- Resembles two superposed one-sided tests
- Decisions for superiority, inferiority, approximate equivalence
|
|
31
|
- Reject hypothesis if observed data is rare when that hypothesis is true
- Consider probability of falsely rejecting each hypothesis
- Usually fix type I error at some prescribed level
- Try for high power (low type II error) for some “design alternative”
|
|
32
|
- Define “rare data” for each hypothesis
- Choose test statistic
- Often based on an estimate of treatment effect
- Reject low treatment effect when estimate is so high as to only occur,
say, with 5% probability
|
|
33
|
- Frequentist inference makes probability statements about the
distribution of the data conditional on a presumed treatment effect,
e.g.,
|
|
34
|
- Frequentist inference thus requires knowledge of the sampling
distribution for the estimate of treatment effect
- Sampling distribution under the null
- Necessary and sufficient to have the correct size test
- Sampling distribution under alternatives
- Necessary to compute
- power of tests
- confidence intervals
- optimality of estimators
|
|
35
|
- To compute sampling distribution
- need to know the probability model to obtain
- Formula for
- Definition of hypotheses
- Distribution of under
every hypothesis
|
|
36
|
- In the probability models most often used for frequentist inference, the
sampling distribution is approximately normal
- Fixed sample setting (no early stopping)
- Large samples
|
|
37
|
- Standard frequentist inference is then
- Consistent point estimate
- 100(1-α)% confidence interval
- P value to test
|
|
38
|
- Sample Size Determination
|
|
39
|
- Design study with sufficient precision to be able to reject at least one
hypothesis with high confidence
- Equivalent criteria for rejection
- type I error = type II error
- interval estimate does not contain both the null and alternative
hypotheses
- Asymmetric definitions of rejection
|
|
40
|
- Number of “sampling units” to obtain desired precision
|
|
41
|
- Often (usually?) logistical constraints impose a maximal sample size
- Compute power to detect specified alternative
- Compute alternative detected with high power
|
|
42
|
- Having chosen a sample size, we can compute
- Threshold for declaring statistical significance
|
|
43
|
- We can also anticipate the inference we will make if we observe an
estimate exactly at the threshold
- P value equal to type I error
- Confidence interval
|
|
44
|
- Evaluation of
- Fixed Sample Clinical
- Trial Designs
|
|
45
|
- Process of choosing a trial design
- Define candidate design
- Usually constrain two operating characteristics
- Type I error, power at design alternative
- Type I error, maximal sample size
- Evaluate other operating characteristics
- Different criteria of interest to different investigators
- Modify design
- Iterate
|
|
46
|
- Frequentist power curve
- Type I error (null) and power (design alternative)
- Sample size requirements
- Threshold for statistical significance
- Frequentist inference at threshold
- Point estimate
- Confidence interval
- P value
|
|
47
|
|
|
48
|
- Consider
- Feasibility of accrual
- Credibility of results
- “3 over n rule”: We may have missed an important subgroup with
different response patterns
- When combined with results from earlier trials
|
|
49
|
- Probability of rejecting null for arbitrary alternatives
- Type I error (power under null)
- Power for specified alternative
- Alternative rejected by design
- Alternative for which study has high power
- Interpretation of negative studies
|
|
50
|
- Threshold for declaring statistical significance
- On the scale of estimated treatment effect
- Assess clinical importance
- Assess economic importance
|
|
51
|
- Inference on the boundary for statistical significance
- Frequentist
- Point estimates
- Confidence intervals
- P values
|
|
52
|
- Sequential Sampling:
- Stopping Rules
|
|
53
|
- Ethical and efficiency concerns are addressed through sampling which
might allow early stopping
- During the conduct of the study, data are analyzed and reviewed at
periodic intervals
- Using interim estimates of treatment effect
- Decide whether to continue the trial
- If continuing, decide on any modifications to sampling scheme
|
|
54
|
- Results convincing for specific hypotheses
- Superiority, approximate equivalence, inferiority
- Results suggestive of inability to ultimately establish a hypothesis of
interest
- No advantage in continuing
- No need to collect additional data on safety, longer term follow-up,
other secondary endpoints
|
|
55
|
- Extreme estimates of treatment effect
- Curtailment:
- Boundary reached early
- Stochastic Curtailment: High probability that a particular decision
will be made at final analysis
- Group sequential test:
- Formal decision rule in classical frequentist framework controlling
experimentwise error
- Bayesian analysis:
- Posterior probability of hypothesis is high
|
|
56
|
- Analyses when sample sizes N1,…, NJ
- Can be randomly determined
- At jth analysis choose stopping boundaries
- Compute test statistic T(X1 ,…, XNj)
- Stop if T < aj (extremely low)
- Stop if bj < T < cj (approximate equivalence)
- Stop if T > dj (extremely high)
- Otherwise continue (with possible adaptive modification of analysis
schedule, sample size, etc.)
|
|
57
|
- Prespecified stopping guidelines
- Adaptive procedures
|
|
58
|
- Prior to first analysis of data, specify
- Rule for determining maximal statistical information
- E.g., fix power, maximal sample size, or calendar time
- Rule for determining schedule of analyses
- E.g., according to sample size, statistical information, or calendar
time
- Rule for determining conditions for early stopping
- E.g., boundary shape function for stopping boundaries on the scale of
some test statistic
|
|
59
|
- A stopping rule for one test statistic is easily transformed to a
stopping rule for another
- “Group sequential stopping rules”
- Sum of observations
- Point estimate of treatment effect
- Normalized (Z) statistic
- Fixed sample P value
- Error spending function
- Conditional probability
- Predictive probability
- Bayesian posterior probability
|
|
60
|
- Parameterization of boundary shape functions facilitates search for
stopping rules
- Can be defined for any boundary scale
|
|
61
|
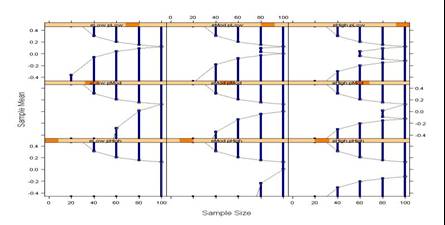
- Down columns: Early vs no early stopping
- Across rows: One-sided vs two-sided decisions
|
|
62
|
- A wide variety of boundary shapes possible
- All of the rules depicted have the same type I error and power to
detect the design alternative
|
|
63
|
- At each analysis of the data, the sampling plan can be modified to
account for changed perceptions of possible results
- E.g., Proschan & Hunsberger (1995)
- Use conditional power considerations to modify ultimate sample size
- E.g., Self-designing Trial (Fisher, 1998)
- Prespecify weighting of groups “just in time”
- Weighting for each group only need be specified at immediately
preceding analysis
|
|
64
|
- Adaptive sampling plans are less efficient
- Tsiatis & Mehta (2002)
- A classic prespecified group sequential stopping rule can be found
that is more efficient than a given adaptive design
- Shi & Emerson (2003)
- Fisher’s test statistic in the self-designing trial provides markedly
less precise inference than that based on the MLE
- To compute the sampling distribution of the latter, the sampling plan
must be known
|
|
65
|
- Full knowledge of the sampling plan is needed to assess the full
complement of frequentist operating characteristics
- In order to obtain inference with maximal precision and minimal bias,
the sampling plan must be well quantified
- (Note that adaptive designs using ancillary statistics pose no special
problems if we condition on those ancillary statistics.)
|
|
66
|
- Frequentist operating characteristics are based on the sampling
distribution
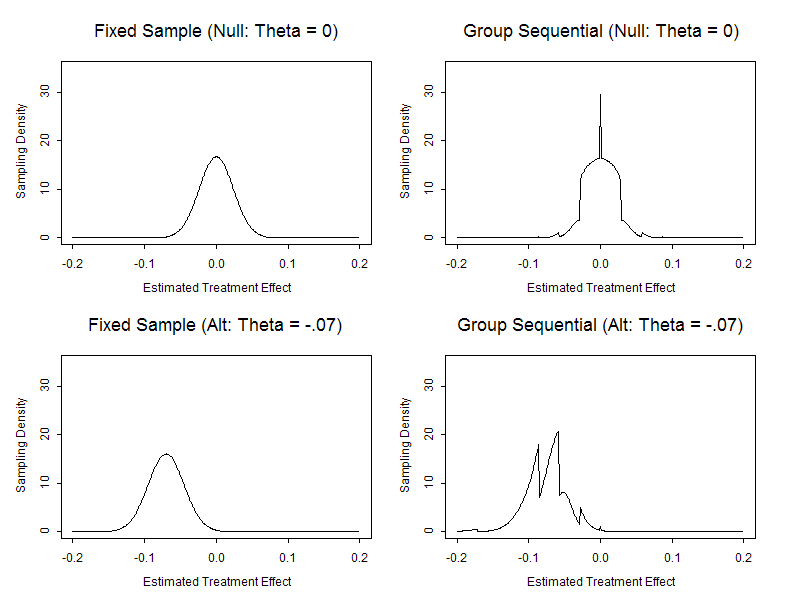
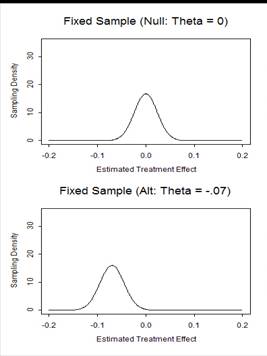
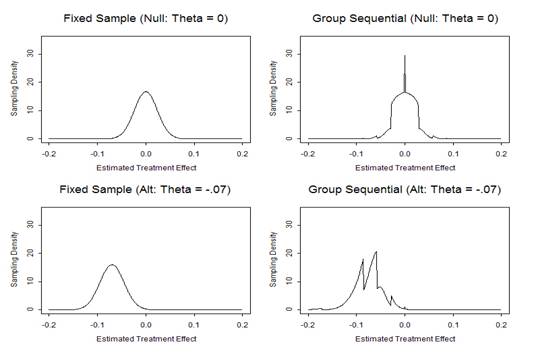
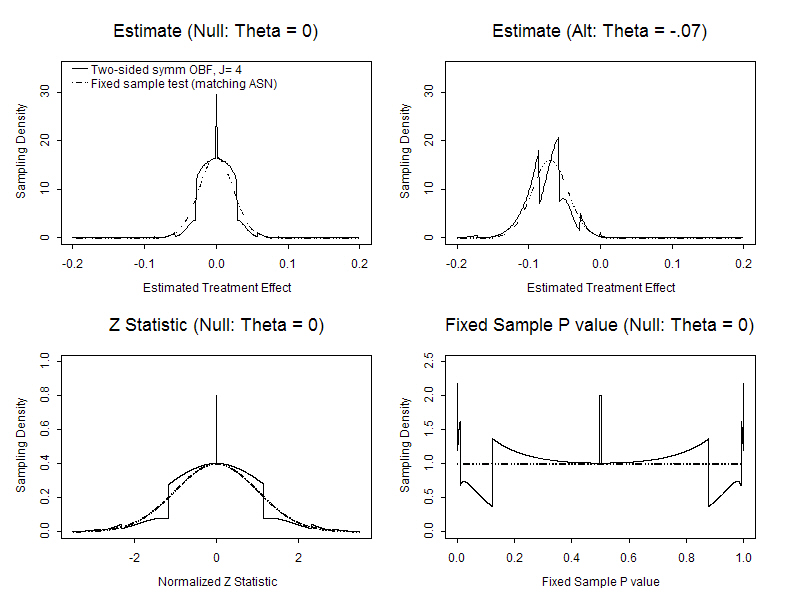
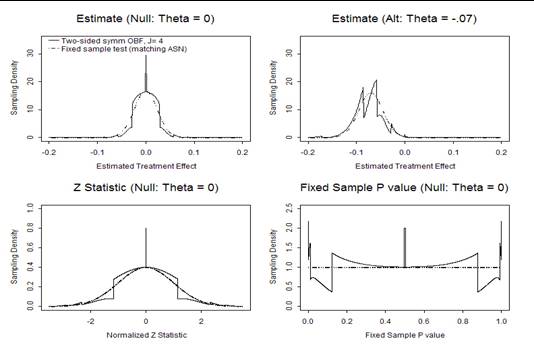
- Stopping rules do affect the sampling distribution of the usual
statistics
- MLEs are not normally distributed
- Z scores are not standard normal under the null
- The null distribution of fixed sample P values is not uniform
- (They are not true P values)
|
|
67
|
|
|
68
|
|
|
69
|
|
|
70
|
- For any stopping rule we can compute the correct sampling distribution
and obtain
- Power curves
- Sample size distribution
- Bias adjusted estimates
- Correct (adjusted) confidence intervals
- Correct (adjusted) P values
- Candidate designs can then be compared with respect to their operating
characteristics
|
|
71
|
- Design stage
- Satisfy desired operating characteristics
- E.g., type I error, power, sample size requirements
- Monitoring stage
- Flexible implementation of the stopping rule to account for
assumptions made at design stage
- E.g., sample size adjustment to account for observed variance
- Analysis stage
- Providing inference based on true sampling distribution of test
statistics
|
|
72
|
- “You better think
(think)
- think about what
you’re
- trying to do…”
- - Aretha
Franklin
|
|
73
|
- Evaluation of
- Group Sequential
- Clinical Trial Designs
|
|
74
|
- Randomized, placebo controlled Phase III study of antibody to endotoxin
- Intervention: Single administration
- Endpoint: Difference in 28 day mortality rates
- Placebo arm: estimate 30% mortality
- Treatment arm: hope for 23% mortality
- Analysis: Large sample test of binomial proportions
- Frequentist based inference
- Type I error: one-sided 0.025
- Power: 90% to detect θ < -0.07
- Point estimate with low bias, MSE; 95% CI
|
|
75
|
- Process of choosing a trial design
- Define candidate design
- Usually constrain two operating characteristics
- Type I error, power at design alternative
- Type I error, maximal sample size
- Evaluate other operating characteristics
- Different criteria of interest to different investigators
- Modify design
- Iterate
|
|
76
|
- Same general operating characteristics of interest no matter the type of
stopping rule
- Frequentist power curve
- Type I error (null) and power (design alternative)
- Sample size requirements
- Maximum, average, median, other quantiles
- Stopping probabilities
- Inference at each boundary
- Frequentist point estimate, confidence interval, P value
- Futility measures
- Conditional power, predictive power
|
|
77
|
- Sample size a random variable
- Summary measures of distribution as a function of treatment effect
- maximum (feasibility of accrual)
- mean (Average Sample N- ASN)
- median, quartiles
- Stopping probabilities
- Probability of stopping at each analysis as a function of treatment
effect
- Probability of each decision at each analysis
|
|
78
|
- Probability of rejecting null for arbitrary alternatives
- Level of significance (power under null)
- Power for specified alternative
- Alternative rejected by design
- Alternative for which study has high power
- Interpretation of negative studies
|
|
79
|
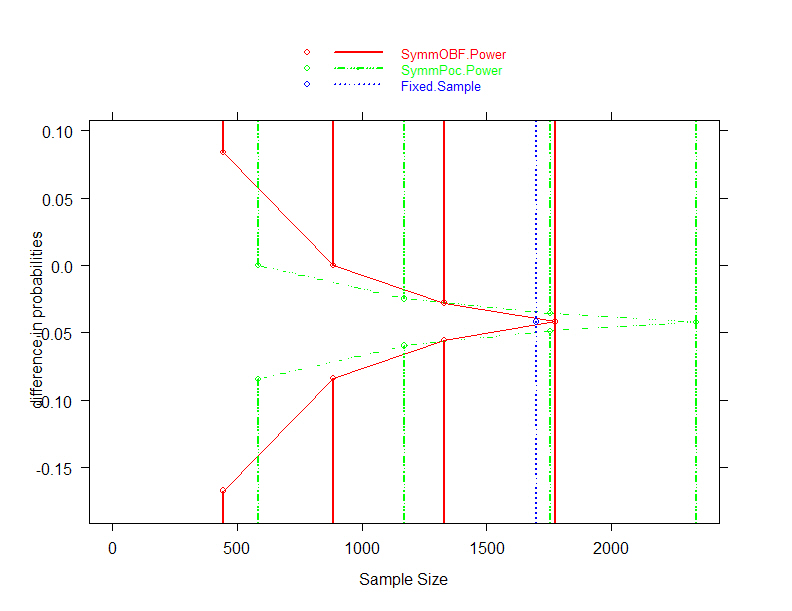
- O’Brien-Fleming, Pocock boundary shape functions when J= 4 analyses
and maintain power
|
|
80
|
- Required increased maximal sample size in order to maintain power
- Maximal sample size with 4 analyses
- O’Brien-Fleming: N= 1773 (
4.3% increase)
- Pocock : N= 2340 (37.6% increase)
- Need to consider
- Average sample size
- Probability of continuing past 1700 subjects
- Conditions under which continue past 1700 subjects
|
|
81
|
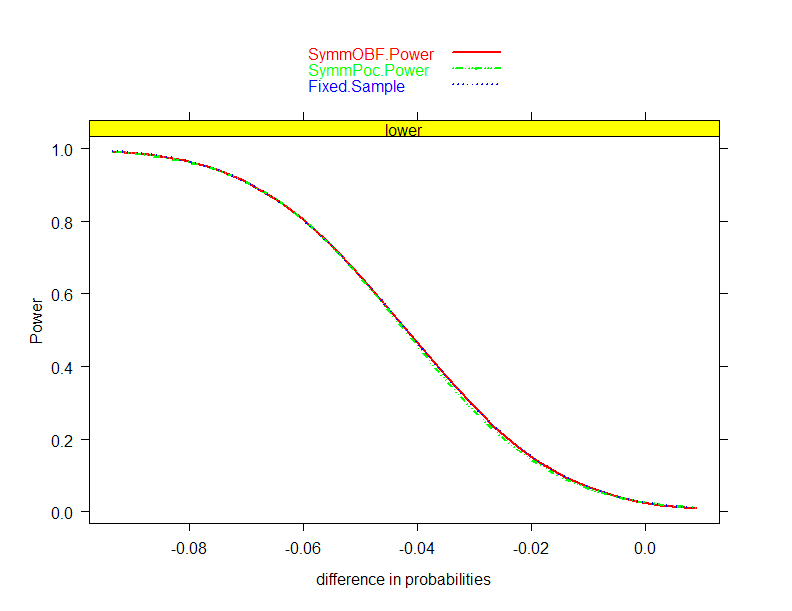
- O’Brien-Fleming, Pocock boundary shape functions;J=4 analyses and
maintain power
|
|
82
|
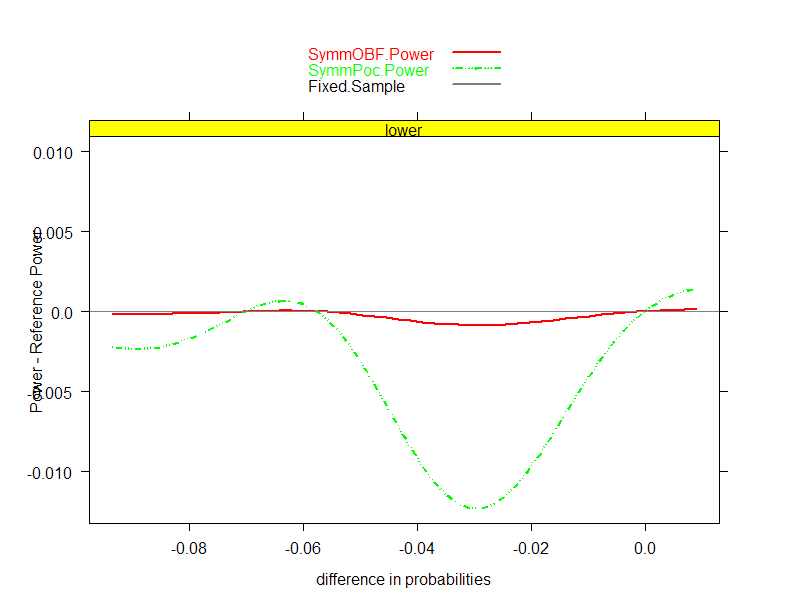
- O’Brien-Fleming, Pocock boundary shape functions when J=4 analyses and
maintain power
|
|
83
|
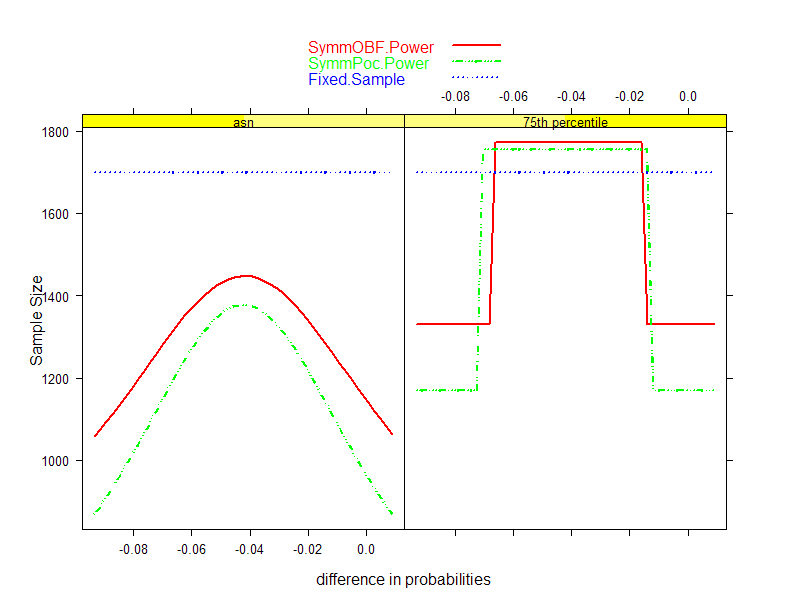
- Increased maximal sample size actually afforded better efficiency on
average
- Pocock boundary shape function: lower ASN over range of alternatives
examined
- This improved behavior despite the 36.7% increase in maximal sample
size
- Worst case behavior
- O’Brien-Fleming: never more than N= 1773
- Pocock continues past 1755 only if MLE for treatment effect is
between -0.0357 and -0.0488
- Always less than 16.01% chance, which occurs when the difference in
mortality is -0.0422
|
|
84
|
- Sponsor preferred not to increase maximal sample size beyond N= 1700
- When investigating the boundaries, the sponsor was surprised to find
that a difference of -0.042 would be statistically significant
- No one had informed the clinical and management teams of the boundary
for the fixed sample test
- Such an effect was only of borderline clinical importance
|
|
85
|
- OBF, Poc boundary shape functions when J= 2, 3, or 4 analyses and
maintain N = 1700
|
|
86
|
- Stopping boundary at each analysis
- On the scale of estimated treatment effect
- Inform DMC of precision
- Assess ethics
- May have prior belief of unacceptable levels
- Assess clinical, economic importance
- On the Z, fixed sample P value, or error spending scales
|
|
87
|
|
|
88
|
- Inference on the boundary at each analysis
- Frequentist
- Adjusted point estimates
- Adjusted confidence intervals
- Adjusted P values
|
|
89
|
|
|
90
|
- Probability that a different decision would result if trial continued
- Compare unconditional power to fixed sample test with same sample size
- Conditional power
- Assume specific hypotheses
- Assume current best estimate
- Predictive power
- Assume Bayesian prior distribution
|
|
91
|
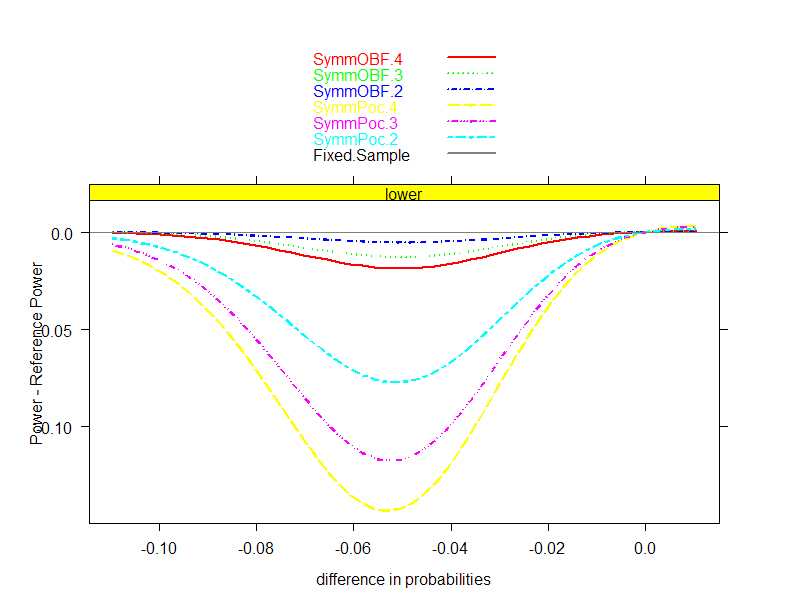
- Sponsor desired greater efficiency when treatment effect is low
- Explored asymmetric designs with a range of boundary shape functions
from unified family
- P= 0.5 (Pocock), 0.8, 0.9, 1.0 (O’Brien-Fleming)
- Compare unconditional power and ASN curves
- Rationale: Are we losing power by stopping early?
- If not, then we are not making bad futility decisions on average
|
|
92
|
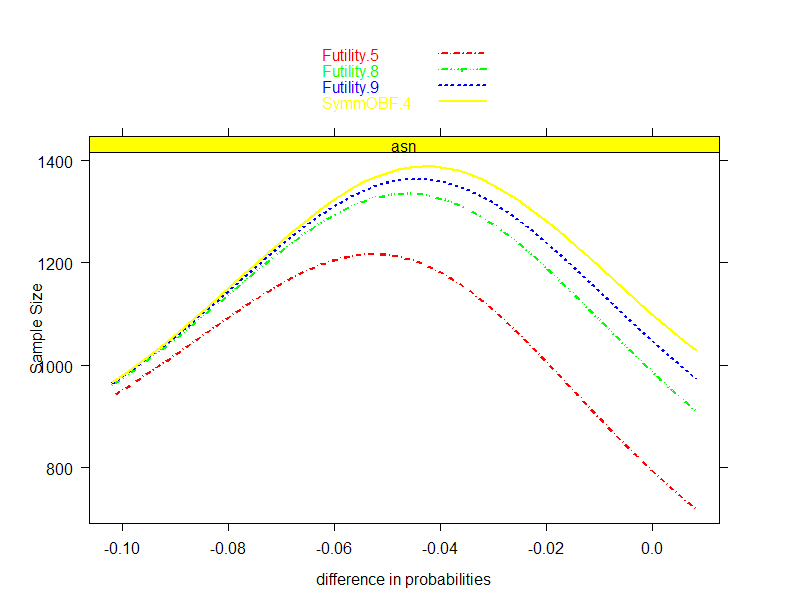
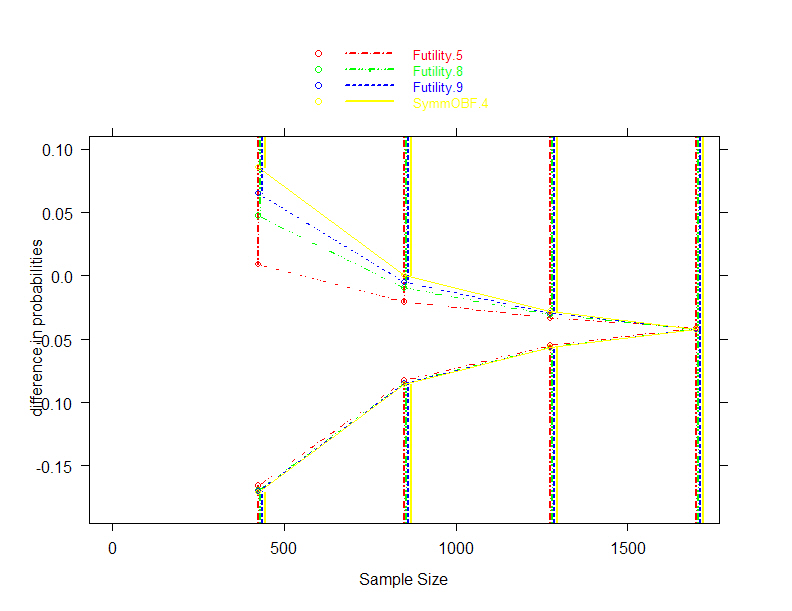
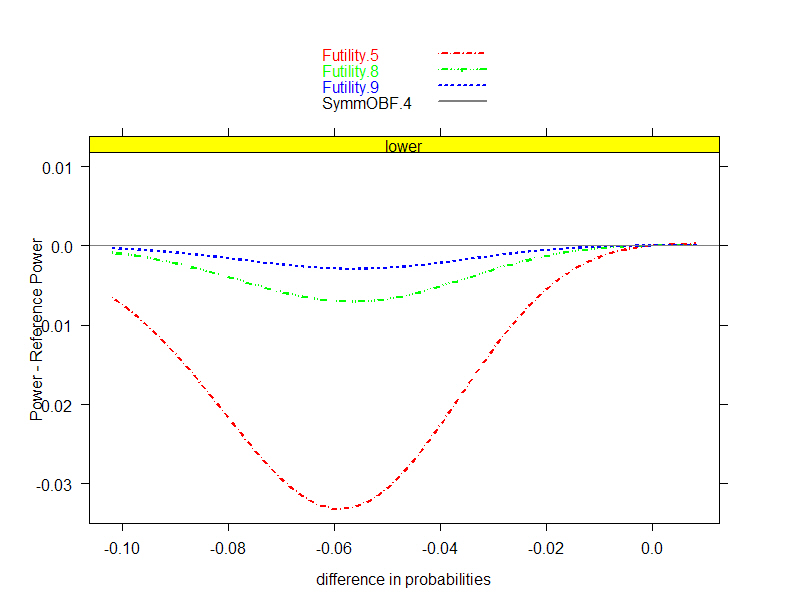
- O’Brien-Fleming efficacy, spectrum of futility boundaries; J= 4
analyses and N=1700
-
Power
- Boundaries (Relative to
Symmetric OBF)
ASN
|
|
93
|
- Sponsor opted for futility boundary based on P= 0.8
- Power – ASN tradeoff
- Worst case loss of power .0071
- (from 0.738 to 0.731 when difference in mortality is -0.0566)
- 10.2% gain in average efficiency under null
- (ASN from 1099 to 987 when difference in mortality is 0.00)
|
|
94
|
- We are sometimes asked about stochastic curtailment
- Boundaries can be expressed on conditional power and predictive power
scales
- Conditional power:
- Probability of later reversing the potential decision at interim
analysis by conditioning on interim results and presumed treatment
effect
- Predictive power:
- Like conditional power, but use a Bayesian prior for the presumed
treatment effect
|
|
95
|
- Key issue: Computations are based on assumptions about true treatment
effect
- Conditional power
- “Design”: assume hypothesis being rejected
- (assumes observed data is relatively misleading)
- “Estimate”: assume that current data is representative
- (assumes observed data is exactly accurate)
- Predictive power
- “Prior assumptions”: Use Bayesian prior distribution
- “Sponsor”: Centered at -0.07; plus/minus SD of 0.02
- “Noninformative”
|
|
96
|
|
|
97
|
- Very different probabilities based on assumptions about true treatment
effect
- Extremely conservative O’Brien-Fleming boundaries correspond to
conditional power of 50% (!) under alternative rejected by the
boundary
- Resolution of apparent paradox: if the alternative were true, there is
less than .0001 probability of stopping for futility at the first
analysis
|
|
98
|
- Neither conditional power nor predictive power have good foundational
motivation
- Frequentists should use Neyman-Pearson paradigm and consider optimal
unconditional power across alternatives
- Bayesians should use posterior distributions for decisions
|
|
99
|
- My experience
- I have consulted with many researchers on successive clinical trials
- Often I am asked about stochastic curtailment the first time
- Never have I been asked about it on the second trial
|
|
100
|
- Probability of obtaining estimates of treatment effect with clinical
(and therefore marketing) appeal
- Modified power curve
- Unconditional
- Conditional at each analysis
- Predictive probabilities at each analysis
|
|
101
|
- Potential to have statistically significant treatment effect estimate of
-0.06 or better
- O’Brien-Fleming efficacy boundary at third analysis:
- Terminate if bias adjusted estimate -0.055 or better
- What is the chance of obtaining -0.06 or better at the fourth analysis
if study continues?
- If true effect is -0.07, probability of 4.1% of BAM < -0.06
- If true effect is -0.06, probability of 3.6% of BAM < -0.06
|
|
102
|
- Modify third analysis efficacy boundary to correspond to BAM of -0.06 or
better
- Probability of BAM < -0.06 increases
- If true effect is -0.07: from 66.6% to 68.6%
- If true effect is -0.06: from 50.4% to 54.0%
|
|
103
|
- Adaptive designs versus prespecified stopping rules
- Adaptive designs come at a price of efficiency
- With careful evaluation of designs, there is little need for adaptive
designs
- Everything I showed today was known prior to collecting any data in
the clinical trial
- Prespecified stopping rules can be chosen which find best tradeoffs
among the various collaborators’ optimality criteria
|
|
104
|
- We have not yet verified that the clinical trial design will be judged
credible by a sufficiently large segment of the scientific community
- Bayesians do not regard frequentist inference as relevant
- We thus need to consider how to evaluate the Bayesian operating
characteristics
|
|
105
|
|
|
106
|
- Frequentist inference considers the distribution of the data conditional
on a presumed (fixed) treatment effect
|
|
107
|
- In the Bayesian paradigm, the parameter measuring treatment effect is
regarded as a random variable
- A prior distribution for
reflects
- Knowledge gleaned from previous trials, or
- Frequentist probability of investigators’ behavior, or
- Subjective probability of treatment effect
|
|
108
|
- Bayes’ rule is used to update beliefs about parameter distribution
conditional on the observed data
|
|
109
|
- Bayesian inference is then based on the posterior distribution
- Point estimates:
- A summary measure of the posterior probability distribution (mean,
median, mode)
- Interval estimates:
- Set of hypotheses having the highest posterior density
- Decisions (tests):
- Reject a hypothesis if its posterior probability is low
- Quantify the posterior probability of the hypothesis
|
|
110
|
- Information required for inference
- Frequentist
- Tests: need the sampling distribution under the null
- Estimates: need the sampling distribution under all hypotheses
- Bayesian
- Tests and estimates: need the sampling distribution under all
hypotheses and a prior distribution
|
|
111
|
- Frequentist
- A precise (objective) answer to not quite the right question
- Well developed nonparametric and moment based analyses (e.g., GEE)
- Conciseness of presentation
- Bayesian
- A vague (subjective) answer to the right question
- Adherence to likelihood principle in parametric settings (and
coarsened approach)
|
|
112
|
- Bayesian:
- Knows the probability that I might be a cheater based on information
derived prior to observing me play
- Knows the probability that I would get 4 full houses for every level
of cheating that I might engage in
- Computes the posterior probability that I was not cheating
(probability after observing me play)
- If that probability is low, calls me a cheater
|
|
113
|
- Frequentist:
- Hypothetically assumes I am not a cheater
- Knows the probability that I would get 4 full houses if I were not a
cheater
- If that probability is sufficiently low, calls me a cheater
- Even if the frequentist dealt the cards!
|
|
114
|
- I take the view that both approaches need to be accomodated in every
analysis
- Goal of the experiment is to convince the scientific community, which
likely includes believers in both standards for evidence
- Bayesian priors should be chosen to reflect the population of priors in
the scientific community
|
|
115
|
- Joint distribution for data and parameter
- Frequentist considers
- Bayesian considers
|
|
116
|
- Choice of probability model for data
- For unified approach to make sense, the frequentist and Bayesian should
use the same conditional distribution of the data
- “Law of the Unconscious Frequentist”:
- Gravitate toward models with good nonparametric behavior
- Choice of prior distributions
- Everyone brings their own
|
|
117
|
|
|
118
|
- Parametric, semiparametric, and nonparametric models for two samples
- My definition of semiparametric models is a little stronger than some
statisticians
- The distinction is to isolate models with assumptions that I think too
strong
- Notation for two sample probability model
|
|
119
|
- F, G are known up to some finite dimensional parameter vectors
|
|
120
|
|
|
121
|
- Forms of F, G are unknown, but related to each other by some finite
dimensional parameter vector
- G can be determined from F and a finite dimensional parameter
- (Most often: Under the null hypothesis, F = G)
|
|
122
|
|
|
123
|
|
|
124
|
- Forms of F, G are completely arbitrary and unknown
- An infinite dimensional parameter is needed to derive the form of G
from F
- (Sometimes we consider “nonparametric families with restrictions”,
e.g., stochastic ordering)
|
|
125
|
|
|
126
|
- In the development and (especially) teaching of statistical models,
parametric models have received undue emphasis
- Examples:
- t test is typically presented in the context of the normal probability
model
- theory of linear models stresses small sample properties
- random effects specified parametrically
- Bayesian (and especially hierarchical Bayes) models are replete with
parametric distributions
|
|
127
|
- Incorrect parametric assumptions can lead to incorrect statistical
inference
- Precision of estimators can be over- or understated
- Hypothesis tests do not attain the nominal size
- Hypothesis tests can be inconsistent
- Even an infinite sample size may not detect the alternative
- Interpretation of estimators can be wrong
|
|
128
|
- (Semi)parametric models are not typically in keeping with the state of
knowledge as an experiment is being conducted
- The assumptions are more detailed than the hypothesis being tested,
e.g.,
- Question: How does the intervention affect the first moment of the
probability distribution?
- Assumption: We know how the intervention affects the 2nd, 3rd, …,
∞ central moments of the probability distribution.
|
|
129
|
- Which null hypothesis should we test?
- The intervention has no effect whatsoever
- The intervention has no effect on some summary measure of the
distribution
|
|
130
|
- What should the distribution of the data under the alternative
represent?
- Counterfactual
- An imagined form for F(t), G(t) if something else were true
- Empirical
- The most likely distribution of the data if the alternative hypothesis
about were true
|
|
131
|
- The null hypothesis of greatest interest is rarely that a treatment has
no effect
- Bone marrow transplantation
- Women’s Health Initiative
- National Lung Screening Trial
- The empirical alternative is most in keeping with inference about a
summary measure
|
|
132
|
- The above views have important ramifications regarding the computation
of standard errors for statistics under the null
- Permutation tests (or any test which presumes F=G under the null) will
generally be inconsistent
|
|
133
|
- Many mechanisms would seem to make it likely that the problems in which
a fully parametric model or even a semiparametric model is correct
constitute a set of measure zero
- Exception: independent binary data must be binomially distributed in
the population from which they were sampled randomly (exchangeably?)
|
|
134
|
- Example 1: Cell proliferation in cancer prevention
- Within subject distribution of outcome is skewed (cancer is a focal
disease)
- Such skewed measurements are only observed in a subset of the subjects
- The intervention affects only hyperproliferation (our ideal)
|
|
135
|
- Example 2: Treatment of hypertension
- Hypertension has multiple causes
- Any given intervention might treat only subgroups of subjects (and
subgroup membership is a latent variable)
- The treated population has a mixture distribution
- (and note that we might expect greater variance in the group with the
lower mean)
|
|
136
|
- Example 3: Effects on rates
- The intervention affects rates
- The outcome measures a cumulative state
- Arbitrarily complex mean-variance relationships can result
|
|
137
|
- Model checking is apparently used by many to allow them to believe that
their models are correct.
- From a recent referee’s report:
- “I know of no sensible statistician (frequentist or Bayesian) who does
not do model checking.”
- Apparently the referee believes the following unproven proposition:
- If we cannot tell the model is wrong, then statistical inference under
the model will be correct
|
|
138
|
- Counter example: Exponential vs Lognormal medians
- Pretest with Kolmogorov-Smirnov test (n=40)
- Power to detect wrong model
- Coverage of 95% CI under wrong model
|
|
139
|
- Model checking particularly makes little sense in a regulatory setting
- Commonly used null hypotheses presume the model fits in the absence of
a treatment effect
- Frequentists would be testing for a treatment effect as they do model
checking
- Bayesians should model any uncertainty in the distribution
- Interestingly, if one does this, the estimate indicating parametric
family will in general vary with the estimate of treatment effect
|
|
140
|
- Impact on what we teach about optimality of statistical models
- Clearly, parametric theory may be irrelevant in an exact sense (though
as guidelines it is still useful)
- Much of what we teach about the optimality of nonparametric tests is
based on semiparametric models
- e.g., Lehmann, 1975: location-shift models
|
|
141
|
- Common teaching:
- A nonparametric alternative to the t test
- Not too bad against normal data
- Better than t test when data have heavy tails
- (Some texts refer to it as a test of medians)
|
|
142
|
- More accurate guidelines:
- In the general case, the t test and the Wilcoxon are not testing the
same summary measure
- Wrong size as a test of Pr(X > Y) unless you assume a
semi-parametric model on some scale
- Inconsistent test of F(t) = G(t)
- (And the Wilcoxon is not transitive)
- Efficiency results when a shift model holds for some monotonic
transformation of the data
- If propensity to outliers is different between groups, the t test may
be better even with heavy tails
- (The variance can be modified to achieve consistency)
|
|
143
|
- The summary measure (functional) measuring treatment effect is just some
difference between distributions
- (Almost always, the problem is ultimately reduced to a 1-dimensional
statistic)
|
|
144
|
- Typical approaches to compare response across two treatment arms
- Difference / ratio of means (arithmetic, geometric, …)
- Difference / ratio of medians (or other quantiles)
- Median difference of paired observations
- Difference / ratio of proportion exceeding some threshold
- Ratio of odds of exceeding some threshold
- Ratio of instantaneous risk of some event
- Probability that a randomly chosen measurement from one population
might exceed that from the other
- …
|
|
145
|
- We thus want to find nonparametric models which
- Include commonly chosen parametric models
- Can be implemented in a Bayesian setting
- It is useful to consider how (semi)parametric models are actually used
|
|
146
|
- How are (semi)parametric assumptions really used in statistical models?
- Choice of functional for comparisons
- Formula for computing the estimate of the functional
- Distributional family for the estimate
- Mean-variance relationship across alternatives
- Shape of distribution for data
|
|
147
|
- Parametric: Driven by efficiency of functional for the particular
parametric family
- Normal: use mean
- Lognormal: use (log) geometric mean
- Double exponential: use median
- Uniform: use maximum
- Semiparametric: Choose functional for scientific relevance, etc., then
adopt a semiparametric model in which desired functional is basic to
model
- Survival data: consider hazard ratio and use proportional hazards
|
|
148
|
- Better bases for choosing summary measure for decisions in order of
importance (nonparametric)
- Current state of scientific knowledge
- Scientific (clinical) relevance
- Potential for intervention to affect the measure
- Statistical accuracy and precision of analysis
|
|
149
|
- How are (semi)parametric assumptions really used in statistical models?
- Choice of functional for comparisons
- Formula for computing the estimate of the functional
- Distributional family for the estimate
- Mean-variance relationship across alternatives
- Shape of distribution for data
|
|
150
|
- Parametric: Estimate parameters and then derive summary measures from
parametric model
- E.g., estimating the median
- Normal: estimate mean; median=mean
- Exponential: estimate mean; median = mean / log(2)
- Lognormal: estimate geometric mean; median = geometric mean
|
|
151
|
- Semiparametric:
- Parameter is fundamental to probability model
- Use both groups to estimate parameter using the assumption that we can
transform one group by the parameter and obtain the same distribution
as the other group
- E.g., proportional hazards model
- Hazard ratio estimate is average of hazard ratios at each failure
time
|
|
152
|
- Survival cure model (Ibrahim, 1999, 2000)
- Probability model
- Proportion πi is cured (survival probability 1 at
∞) in the i-th treatment group
- Noncured group has survival distribution modeled parametrically
(e.g., Weibull) or semiparametrically (e.g., proportional hazards)
- Treatment effect is measured by θ = π1 – π0
- The problem as I see it: Incorrect assumptions about the nuisance
parameter can bias the estimation of the treatment effect
|
|
153
|
- Nonparametric: Estimate summary measures from nonparametric empirical
distribution functions
- E.g., use sample median for inference about population medians
- Often the nonparametric estimate agrees with a commonly used
(semi)parametric estimate
- Interpretation may depend on sampling scheme
- In this case, the difference will come in the computation of the
standard errors
|
|
154
|
- How are (semi)parametric assumptions really used in statistical models?
- Choice of functional for comparisons
- Formula for computing the estimate of the functional
- Distributional family for the estimate
- Mean-variance relationship across alternatives
- Shape of distribution for data
|
|
155
|
- Parametric: Use probability theory to derive distribution of estimate
- E.g., estimating the median
- Normal: sample mean is normal
- Exponential: sum is gamma
- Lognormal: log geometric mean is normal
- Semiparametric:
- Small sample properties: Conditional distributions based on
permutation
- Large sample properties: Asymptotics
|
|
156
|
- Nonparametric: Asymptotic normal theory (almost always)
- Most nonparametric estimators involve a sum somewhere
- Central limit theorem holds (like it or not)
- Thus gamma distributions converge to a normal…
|
|
157
|
- How are (semi)parametric assumptions really used in statistical models?
- Choice of functional for comparisons
- Formula for computing the estimate of the functional
- Distributional family for the estimate
- Mean-variance relationship across alternatives
- Shape of distribution for data
|
|
158
|
- Asymptotically, most summary measures have a limiting normal
distribution (exception is the supremum of the difference between the
cdf’s)
- In this setting, we need only estimate the variance of the sampling
distribution under specific hypotheses
- Formulas
- Bootstrapping within groups (Population model)
- Permutation distributions (Randomization model)
|
|
159
|
|
|
160
|
- In most cases, however, it must be recognized that we can only estimate
the variance under the truth, which may not correspond to a hypothesis
of interest
- If the intervention can affect the variance of the summary measures,
then we must account for a mean-variance relationship when considering
different hypotheses
|
|
161
|
- Example: Two sample test of binomial proportion
|
|
162
|
- Two sample test of binomial proportion
- Estimated variance is subject to
- Sampling variability
- Difference between the truth and the hypothesis
|
|
163
|
- Estimating mean variance relationships
- May not be too important for frequentist tests of the null hypothesis,
because convention often dictates the null variance we should use
- Use randomization and/or population variances in adversarial argument
- However confidence intervals and all Bayesian inference are statements
about what data would arise under a variety of hypotheses
- We must have some idea about how the variance might change with the
mean
|
|
164
|
- Possible approaches to the mean-variance relationship estimation
- Explore various mean-variance relationships
- Bootstrap tilting could be used here
- Assume no mean-variance relationship
- Sensitivity analyses intermediate to the two
|
|
165
|
- A key issue is deciding how many observations are present for estimating
the mean-variance relationship
- If the control group can be used to estimate behavior under the null
and the treatment group under the alternative, then possibly have two
- If an active intervention modifies the response in both groups or in
population model, then may only have one
|
|
166
|
- How are (semi)parametric assumptions really used in statistical models?
- Choice of functional for comparisons
- Formula for computing the estimate of the functional
- Distributional family for the estimate
- Mean-variance relationship across alternatives
- Shape of distribution for data
|
|
167
|
- Shape of distribution for data
- Only really an issue for prediction, which is not considered here
|
|
168
|
- Nonparametric
- Bayesian Models
|
|
169
|
- Nonparametric Bayesians have focussed primarily on Dirichlet process
priors
- Prior placed on all multinomial distributions
- Can be chosen to include all distributions
- Interpretation of priors is extremely difficult
- How much mass is placed on bimodal distributions?
- Correspondence with frequentist methods?
|
|
170
|
- Modification for nonparametric models
- Use summary measure estimate as the data
- Use asymptotic distributions under population model
|
|
171
|
- If
- the parameter estimate is the sufficient statistic,
- if the estimate is approximately normal, and
- the mean-variance relationship is correct
- Then
- the only difference is using the
approximate normal distribution instead of the parametric form
|
|
172
|
- Same probability model typically used by frequentists
- Robust inference about summary measure
- Specification of prior distributions on the parameter of interest
- Choice of conjugate normals allows conciseness of presentation using
contour plots
|
|
173
|
- The chief advantage of frequentist inference (to my mind) is that it
presents a standard for concise presentation of results
- Estimates, standard errors, P values, CI
- Bayesian analysis requires such a presentation for every prior
- Your prior does not matter to me
- A consensus prior will not capture the diversity of prior opinion
|
|
174
|
- In the context of the coarsened Bayes approach, we can adopt a standard
based on conjugate normal priors
- Two dimensional space of prior distributions
- Prior mean (pessimism)
- Prior standard deviation (dogmatism)
- Also can be measured as information in prior relative to that in
planned sample
|
|
175
|
- Bayesian inference as a contour plot for each inferential quantity
- Posterior mean
- Limits of credible intervals
- Posterior probabilities
- Under sequential sampling, present contour plots for each analysis time
|
|
176
|
|
|
177
|
|
|
178
|
- Advantages and disadvantages of such sensitivity analyses
- To the extent that people can only describe the first two moments of
their prior:
- A convenient standard for presentation
- But, normal prior is less informative than other priors having the
same mean and variance
|
|
179
|
- Mean-variance relationship
- Provide a prior distribution for summary measure that incorporates a
prior on the mean-variance relationship
- Note that the concept of updating the prior is probably not valid here,
because there is really no added information about mean-variance
relationship
- The mean variance relationship is observed at two points (at most)
|
|
180
|
- Ramifications
- The approach to using estimates as the data does mean that in some
cases we cannot regard that we are continually updating our posterior
- E.g.: The sample median of the combined sample is not necessarily a
weighted mean of the sample median from two separate samples
|
|
181
|
- The approach proposed here requires a graph for every number that would
have been reported in a frequentist analysis
- I doubt many editors will agree
- It should be clear, however, that the frequentist nonparametric estimate
and standard error are sufficient for a reader to perform his/her own
sensitivity analysis
|
|
182
|
|
|
183
|
- The driving force in a clinical trial should be a valid scientific
experiment in an ethical manner
- The approach proposed here has placed greatest emphasis on
- robustness, and
- communicability (concise standards)
|
|
184
|
- There are many aspects which could be improved
- Behavior of estimates for mean-variance relationship
- Robustness to “model misspecification”
- e.g., linear contrasts used with nonlinear trends
- Adjustment for covariates
|
|
185
|
- There are some important issues not really addressed at all
- Time-varying treatment effects
- Nonproportional hazards
- Longitudinal data
|
 Notes
Notes{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}